How Long Does It Take for Medicaid to Start Again After the Case Has Been Closed
The COVID-19 pandemic has resulted in authoritative challenges for state Medicaid agencies from staff transitions to telework due to social distancing requirements, increased applications during the economic downturn, and the need to alter policies and procedures to facilitate access to coverage and intendance in response to the public wellness crisis. Equally a result, states have faced increased enrollment while having fewer staff and resources available for routine eligibility and enrollment processing. At the aforementioned time, Maintenance of Eligibility (MOE) provisions crave states to keep beneficiaries enrolled until the cease of the month when the COVID-19 public health emergency (PHE) ends and prohibit states from adopting more stringent eligibility criteria or increasing premiums, every bit weather condition of receiving temporary increased federal Medicaid funding under the Families First Coronavirus Response Act. Consequently, states will demand to address a backlog of Medicaid eligibility renewals and redeterminations equally well equally continue to process new applications after the PHE ends.
In addition, many states accept adopted temporary policy changes through various Medicaid emergency authorities to expand eligibility and/or streamline enrollment processes to connect individuals to coverage more quickly during the pandemic. States also have used emergency government to adopt other policies such equally relaxing price sharing and prior authorization requirements, increasing provider payments, and calculation new benefits. States will have to make up one's mind whether to continue these policy changes after the PHE ends. If states return to pre-PHE eligibility and enrollment rules, they will need to redetermine eligibility for impacted enrollees. They also volition demand to notify beneficiaries and providers about any payment or benefit changes.
On December 22, 2020, CMS released a land wellness official letter outlining how states are expected to unwind emergency authorities and resume normal eligibility and enrollment processing after the finish of the PHE. The current PHE annunciation expires on April 21, 2021, but the Biden Administration has indicated the PHE volition likely remain in place throughout 2021 and that states will receive lx days notice before the end of the PHE to prepare for the finish of emergency regime and the resumption of pre-PHE rules. The change in Presidential administration could have implications for land planning and decisions at the end of the PHE, as the Biden Administration could revise the December 2020 guidance as well as the Trump Administration's interim final dominion (IFR) governing the MOE provisions. Because the Trump Administration did non finalize the IFR following the end of the annotate period in January, the Biden Administration will accept the opportunity to review comments and could make modifications in response to comments before finalizing the rule. This brief highlights key issues from the new CMS guidance to states every bit issued in Dec 2020.
What actions does CMS expect states to take during the PHE?
CMS expects states to process applications, redeterminations and renewals to the extent possible during the PHE, even though they cannot terminate coverage for most enrollees due to the MOE. CMS emphasizes prioritizing actions to ensure that individuals can enroll in and retain coverage, such equally determining eligibility for new applications, during the PHE.one Tabular array 1 summarizes the circumstances that may result in state backlogs and the deportment that CMS expects states to take during the PHE to address pending eligibility and enrollment actions. CMS also encourages states to conduct CHIP and Basic Health Program (BHP) redeterminations and renewals during the PHE. Because the MOE does not employ to those programs, CMS notes that states can procedure Bit and BHP deportment now, which could allow them more time to focus on clearing Medicaid backlogs after the PHE and MOE conditions end.
| Table i: Country Eligibility and Enrollment Backlogs and Expected State Deportment During the PHE | ||
| Type of Action | Circumstances That May Contribute to Backlog When PHE Ends | Actions CMS Expects States to Take During PHE |
| Applications | The economical downturn has led to increased applications, and states may not have finished processing all applications received during the PHE by the time the PHE ends. States also need to go on to process new applications received mail-PHE. | States should make every endeavour to brand timely eligibility determinations for new applicants. |
| Verifications | States that determine eligibility based on self-attested information must complete post-enrollment verification. | States should begin processing pending post-enrollment verifications to the extent possible and resume checking information sources to verify eligibility criteria for those enrolled based on self-attested data. |
| Redeterminations | Some individuals may have gained eligibility due to state-adopted emergency authorities that expanded eligibility (such every bit increased income/asset disregards). States volition take to redetermine eligibility for these enrollees if they revert to prior rules after the PHE ends. Enrollees besides may accept reported changes in circumstances during the PHE, only MOE rules required states to continue coverage. | States should brand every attempt to process changes in circumstances that may expand coverage, and process other changes in circumstances to the extent possible. |
| Renewals | States may have delayed processing eligibility renewals that were due during the PHE due to the need to focus on pandemic response. | States should process overdue renewals to the extent possible and initiate renewals based on electronic data/information available to the state. |
| SOURCE: CMS, SHO #20-004, Planning for the Resumption of Normal State Medicaid, Children'due south Wellness Insurance Program (Chip), and Basic Health Plan (BHP) Operations Upon Conclusion of the COVID-nineteen Public Wellness Emergency (December. 22, 2020). | ||
To assist ensure that future workloads are manageable, states can take activity to evenly distribute renewals throughout the year. When completing renewals that were delayed during the PHE on an ex parte basis (using information available to the state and not requiring information from the individual), states take the option to retain the private'southward original eligibility menstruum (effective when the renewal was due) instead of beginning a new eligibility period on the date the renewal really is completed. This may assistance states distribute workloads in future years past staggering renewal dates but may as well upshot in renewal periods for enrollees that are shorter than 12 months.
How quickly does CMS expect states to clear eligibility and enrollment backlogs later the PHE ends?
CMS expects states to consummate all pending eligibility and enrollment actions and articulate any backlogs within half dozen months later on the PHE ends. The guidance sets timelines for states to render to normal operations for eligibility determinations on new applications too as eligibility verifications, redeterminations based on changes in circumstances, and renewals that are pending when the PHE ends (Figure 1). Initial milestones focus on processing applications, followed by completing pending verifications, redeterminations, and renewals.
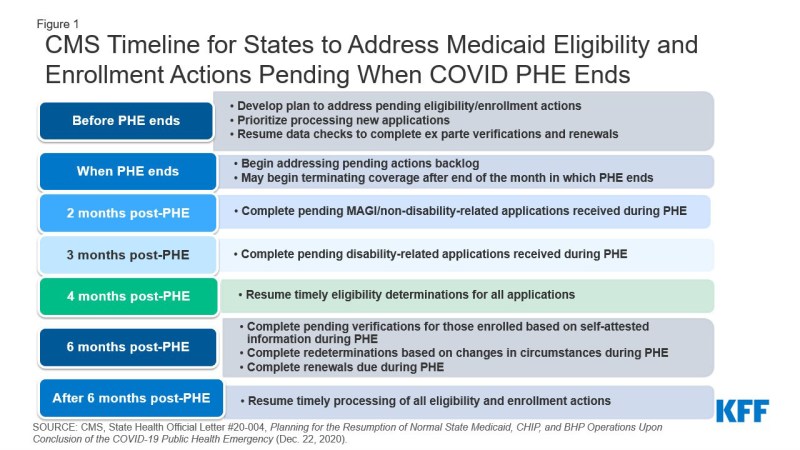
Effigy 1: CMS Timeline for States to Address Medicaid Eligibility and Enrollment Actions Pending When COVID PHE Ends
States need to adopt a methodology for prioritizing which pending eligibility and enrollment actions to complete beginning, focused on individuals "most likely" to no longer be eligible (Table 2).2 States have discretion virtually whether to adopt one of CMS's methodologies or to develop their ain approach. The state'southward methodology will be part of the operational plan that it must develop to set out how information technology volition process pending actions inside CMS-required timeframes afterwards the PHE ends. CMS will not approve land operational plans but may asking them from states that are non coming together the required timeframes. States must submit baseline information about pending eligibility and enrollment actions at the end of the PHE and submit updates quarterly thereafter to testify progress toward the timeframes. If states encounter these timeframes, CMS will not consider eligibility and enrollment actions delayed due to the PHE equally untimely for Program Mistake Charge per unit Measurement (PERM) purposes.3
| Table ii: State Options for Methodology to Prioritize Awaiting Eligibility and Enrollment Deportment | |
| Methodology | Clarification |
| Population-based arroyo | Prioritizes eligibility and enrollment actions for individuals in groups who are most likely to be no longer eligible (due east.m., those who aged out of group, expansion adults who became Medicare-eligible). |
| Time-based approach | Prioritizes deportment based on the length of fourth dimension the activity has been awaiting (state completes oldest pending actions first). |
| Hybrid approach | Combines the population and time-based approaches (east.g. use fourth dimension-based arroyo to prioritize post-enrollment verifications and changes in circumstances and use population-based approach to prioritize renewals; or utilise population-based approach for kickoff moving ridge of pending actions then switch to time-based approach). |
| State-adult approach | Develop another approach that prioritizes deportment for individuals who are about likely to be no longer eligible or that pose a greater risk for ineligible individuals remaining enrolled longer. |
| SOURCE: CMS, SHO #twenty-004, Planning for the Resumption of Normal State Medicaid, Children'due south Health Insurance Program (Flake), and Basic Wellness Program (BHP) Operations Upon Conclusion of the COVID-19 Public Health Emergency (Dec. 22, 2020). | |
The guidance reiterates existing policies states can adopt to streamline eligibility and enrollment processes and reduce authoritative workload. For MAGI populations (whose eligibility is based solely on low income), these options include renewing coverage for 12 months when processing changes in circumstances and a data check shows continued eligibility, relying on income determinations made by SNAP or TANF, as well equally Express Lane Eligibility and 12-month continuous enrollment for children. States can likewise streamline eligibility and renewal processes for not-MAGI enrollees (whose eligibility is based on old age or disability) past adopting 12 calendar month renewal periods, using prepopulated renewal forms, offer renewal reconsideration periods, and modifying verification policies to take cocky-testament, among other policies.4
After the PHE ends, what do states need to practice before terminating coverage?
States cannot terminate coverage until the end of the month in which the PHE ends, due to the MOE requirements. After the MOE and whatever temporary emergency regime end, states must follow regular program rules that require sending x day advance notice and providing the opportunity for a fair hearing prior to terminating coverage. If states are ending emergency government and redetermining eligibility under more than restrictive pre-PHE rules, states must provide enrollees with a reasonable timeframe, at least xxx days, to provide information to establish their connected eligibility.5 States too must ensure a polish transition to other insurance affordability programs for those who lose Medicaid eligibility but may be eligible for Marketplace or other coverage.
After the PHE and MOE requirements terminate, states practise non accept to repeat redeterminations or renewals before terminating coverage for individuals who have been determined ineligible within half-dozen months of the date the state sends an advance detect of coverage termination. To adopt this option, states must inform the enrollee at the time of the ineligibility decision that coverage volition stop after the month in which PHE ends, and the state volition redetermine their eligibility based on any changes in circumstances that they report prior to termination. The state and so must ship a 2d observe in advance of the termination date. In cases where the country requests data to institute connected eligibility, states must allow individuals to answer through the end of the PHE, regardless of when the request was sent. If an individual has not responded to a request that was sent within half-dozen months of the appointment on which the state intends to stop coverage after the PHE ends, the state may transport advance discover of termination without attempting a repeated verification or redetermination.
What do states need to do if they want to keep or end policies adopted through emergency authorities?
The diverse Medicaid emergency authorities adopted during the PHE volition end automatically (when the PHE ends or on a specified end date), unless a state takes activeness to extend them. States are not subject to public detect requirements for returning to pre-PHE rules. Notwithstanding, CMS strongly encourages states to communicate nigh changes with providers, enrollees, and managed care plans. And, states must provide advance notice to enrollees of whatever actions that result in a loss of eligibility, a reduction in benefits, or an increment in toll-sharing; this includes changes due to ending an emergency authority that temporarily expanded eligibility or benefits. Although some states already have sent notices during the PHE informing enrollees of changes that will take consequence after the PHE or MOE ends (such as increased cost-sharing), states must send a 2d accelerate observe at the cease of the PHE prior to implementing these changes.6
CMS encourages states to consider whether some emergency authorities should finish earlier the PHE ends. For example, many states paused Preadmission Screening and Resident Review (PASRR) assessments, which prevent unnecessary nursing facility stays and facilitate customs transitions, for people with intellectual or developmental disabilities or mental illness entering nursing homes during the pandemic. Given PASRR'due south role in preventing unnecessary institutionalization, CMS encourages states to re-start PASRR earlier the PHE ends.7
States may want to proceed some policies adopted under emergency regime subsequently the PHE ends, though not all policies tin be continued. For case, states can amend their country plans or HCBS waivers to go on service commitment via telehealth. States also can update their verification plans to go on streamlined eligibility and enrollment options. CMS specifically encourages states to identify any temporary regime that increased access to HCBS and make these changes permanent. However, states that used Department 1135 waiver authority to relax provider screening requirements and/or temporarily enroll providers who participate in other country Medicaid programs or Medicare must return to regular plan rules. States have six months from the end of the PHE to complete screenings of these provisional providers and to stop payments to any providers non fully enrolled.
CMS is also now allowing states to extend HCBS waiver emergency government adopted under Appendix K up to vi months later the PHE ends. Appendix K allows states to make temporary changes to HCBS waivers in response to emergencies, such as modifying or expanding eligibility or benefits, modifying or suspending service planning and delivery requirements, and adopting policies to support providers. Appendix K approvals to date were scheduled to expire later one year, with the first expirations to occur in late January 2021. Given the pandemic's longevity and incertitude about how long the PHE ultimately will last, CMS is now allowing states to submit requests to extend existing Appendix K approvals upward to six months after the PHE ends and will apply this end date to new Appendix K requests going forrad.8 Afterward vi months post-PHE, states can continue many Appendix K policies by amending their HCBS waivers.9
Source: https://www.kff.org/medicaid/issue-brief/key-issues-for-state-medicaid-programs-when-the-covid-19-public-health-emergency-ends/
0 Response to "How Long Does It Take for Medicaid to Start Again After the Case Has Been Closed"
Post a Comment